


الحمدلله والصلاة والسلام على رسول الله وعلى آله وصحبه أجمعين
Spinal Anesthesia
Spinal anesthesia also called spinal analgesia or sub-arachnoid block (SAB), is a form of regional anaesthesia involving injection of a local anaesthetic into the subarachnoid space, generally through a fine needle, usually 9 cm long (3.5 inches).
Spinal anesthesia is a technique in which the patient is given an injection in the lower back that blocks the nerves that supply feeling to the lower half of the body.
The medication is injected into a sac of fluid in your lower back (the subarachnoid space) which contains the spinal nerves.
The medication blocks the nerves in the lower half of the body. The loss of feeling is temporary and should last from 1 to 4 hours depending on the medication given and other factors
وهي عن طريق حقن ابرة رفيعة جدا وجرعة واحدة في السائل او ال
SUBARACHNOID SPACE اي في السائل المحيط بالحبل الشوكي وهي تحتاج الى نسبة بسيطة جدا من جرعة التخدير لانها تؤدي الى التخدير الجزء السفلي من الجسم

epidural anesthesia, a form of regional anesthesia involving injection of drugs through a catheter placed into the epidural space. The injection can cause both a loss of sensation (anaesthesia) and a loss of pain (analgesia), by blocking the transmission of signals through nerves in or near the spinal cord.
Difference from spinal anesthesia
-The involved space is larger for an epidural, and subsequently the injected dose is larger, being about 10-20 ml in epidural anesthesia compared to 1,5-3,5 ml in a spinal.
-In an epidural, an indwelling catheter may be placed that avails for additional injections later, while a spinal is a one-shot only.
-The onset of analgesia is approximately 15-30 minutes in an epidural, while it is approximately 5 minutes in a spinal.
-An epidural usually doesn't cause significant neuromuscular block, while a spinal more often does. An epidural may be given at a thoracic or lumbar site, while a spinal must be injected below L2 to avoid piercing the spinal cord.
صورة توضح مكان دخول الابرة بين فقرات الظهر في الغضروف بعيدا عن الاعصاب
1- الحقن في وضع الجلوس :
يجلس المريض على منضدة العمليات مريحا قدميه على مقعد صغير مع ثني العمود الفقري بحيث يأخذ الظهر سطحا محدبا وذلك بضغط الذقن على عظمة القص
. فبذلك تبرز الزوائد أو النتوءات الشوكية ( Spinous Processes ) بوضوح كما تتسع المسافة بين الفقرات ويساعد على الوصول إلى هذا الوضع لو ضغطنا أيضا على البطن عند الصرة .
ثم يعقم ويطهر موضع الحقن بصبغة اليود أو الميكركروم الكحولي
- وبعد تجفيف المكان الذي ستؤخز فيه الإبرة الخاصة بالتخدير النصفي ( Spinal Needle ) فتخرق الجلد والأغشية تحت الجلدية ثم الأربطة التي توصل بين نتوءات الفقرات حتى تصل إلى المسافة خارج الام الجافية – ثم الام الجافية والعنكبوتية لتصل إلى المسافة تحت العنكبوتية والتي يجري فيها السائل النخاعي حيث يتم الحقن بالسائل المخدر.
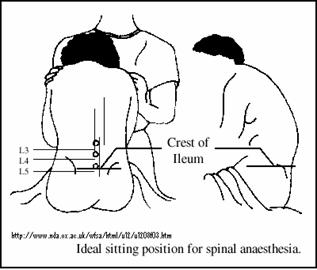
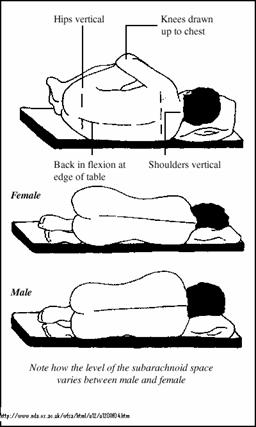
Position of the patient
The patient may be in the sitting position or lateral position (lying on one side). The sitting patient is asked to slouch and bend forward slightly from the waist to increase the curvature of the spine. The lying patient is asked to draw the knees up to the chin for the same reason.
طريقة إعطاء التخدير النصفي
ب- الحقن في الوضع الجانبي :
ينام المريض على جانبه فوق منضدة العمليات بحيث يكون ظهره على حافة المنضدة وتنثني الركبتين على البطن – والرأس إلى الركبتين – مع ملاحظة أن مفاصل الحوض والكتف تكون عمودية على المنضدة - ونختار هذا الوضع إذا أردنا التخدير على جانب واحد من الجسم – وعندئذ يكون جانب المريض هو الملتصق بمنضدة العمليات عند استعمال السوائل المخدرة الثقيلة والجانب السليم هو الملتصق بالمنضدة عند استعمال السوائل المخدرة ذات الثقل النوعي الخفيف
Anaesthetic drugs
A patient receiving an epidural for pain relief typically receives a combination of local anesthetics and opioids. This combination works better than either type of drug used alone. Common local anesthetics include lidocaine, bupivacaine, ropivacaine, and chloroprocaine. Common opioids include morphine, fentanyl, sufentanil, and pethidine . These are injected in relatively small doses
.
Contraindications
Absolute
Patient refusal
Coagulopathy.
Insertion of an epidural needle or catheter into the epidural space may cause traumatic bleeding into the epidural space. Clotting abnormalities may lead to the development of a large haematoma leading to spinal cord compression.
Therapeutic anticoagulation.
( see later)
Skin infection at injection site.
Insertion of the epidural needle through an area of skin infection may introduce pathogenic bacteria into the epidural space, leading to serious complications such as meningitis or epidural abscess.
Raised intracranial pressure.
Accidental dural puncture in a patient with raised ICP may lead to brainstem herniation (coning).
Hypovolaemia.
The sympathetic blockade produced by epidurals, in combination with uncorrected hypovolaemia, may cause profound circulatory collapse.
Relative
Uncooperative patients
may be impossible to position correctly, and be unable to remain still enough to safely insert an epidural.
Pre-existing neurological disorders,
such as multiple sclerosis, may be a contraindication, because any new neurological symptoms may be ascribed to the epidural.
Fixed cardiac output states.
Probably relative rather than absolute. This includes aortic stenosis, hypertrophic obstructive cardiomyopathy (HOCM), mitral stenosis and complete heart block. Patients with these cardiovascular abnormalities are unable to increase their cardiac output in response to the peripheral vasodilatation caused by epidural blockade, and may develop profound circulatory collapse which is very difficult to treat.
Anatomical abnormalities of vertebral column may make the placement of an epidural technically impossible.
Prophylactic low dose heparin
Regional anesthesia and anticoagulants
Full oral anticoagulation with warfarin or standard heparin (SH) are absolute contraindications to epidural blockade.
Partial anticoagulation with low molecular weight heparin (LMWH) or low dose warfarin (INR <1.5) are relative contraindications.
Low dose standard heparin (SH), 5,000units bd s/c is not associated with an increased risk of epidural haematoma. Wait for 4 hours after a dose before performing epidural.
LMWH : allow 12hr interval between LMWH administration and epidural; this also applies to removal of epidural catheters.
NSAID's (including aspirin) do not increase the risk of epidural haematoma.
Intraoperative anticoagulation using 5000units i/v heparin following epidural/spinal injection appears safe, but careful postoperative observations are recommended. .
Fibrinolytic and thrombolytic drugs: avoid epidural block for 24 hrs, check clotting prior to insertion.
Thrombocytopaenia: epidurals are relatively contraindicated below platelet count of 100,000/mm3.
An epidural haematoma should be suspected in patients who complain of severe back pain a few hours/days following any central neuraxial block or with any prolonged or abnormal neurological deficit (including. sensory loss, paraesthesiae, muscle weakness and disturbance of bladder control and anal sphincter tone). A high index of suspicion is required, with early orthopaedic or neurosurgical referral for decompression of the haematoma. Even with early recognition, the morbidity of this condition is still very high
Important complications of regional anaesthesia
Pain - 25% of patients still experience pain despite spinal anaesthesia
Post-dural headache from CSF leak
Hypotension and bradycardia through blockade of the sympathetic nervous system
Limb damage from sensory and motor block
Epidural or intrathecal bleed
Respiratory failure if block is 'too high'
Direct nerve damage
Hypothermia
Damage to the spinal cord - may be transient or permanent
Spinal infection
Aseptic meningitis
Haematoma of the spinal cord - enhanced by use of LMWH preoperatively
Anaphylaxis
Urinary retention
و يتميز التخدير النصفي بما يلي
:
يجنب المريض بعض الآثار السيئة للمواد المستخدمة فى التخدير الكلي و لا سيما فى مرضى القلب و الكبد و الجهاز التنفسي
.
يساعد على تقليل ضغط الدم مما يساعد على تقليل النزف فى جراحات الفخذ (لا يوجد نزف فى جراحات الركبة لأنه يتم وضع رباط على الفخذ يمنع وصول الدم للركبة أثناء الجراحة
).
لا يحتاج المريض لوقت للإفاقة من التخدير و يستطيع الأكل و الشرب بعد إجراء الجراحة مباشرة و لا يوجد ميل للقيء
.
تساعد على تقليل الألم بعد الجراحة حيث يمكن تركيب أنبوب رفيع للغاية يتم من خلاله حقن المواد المخدرة بعد الجراحة
Spinal Anesthesia
Spinal anesthesia also called spinal analgesia or sub-arachnoid block (SAB), is a form of regional anaesthesia involving injection of a local anaesthetic into the subarachnoid space, generally through a fine needle, usually 9 cm long (3.5 inches).
Spinal anesthesia is a technique in which the patient is given an injection in the lower back that blocks the nerves that supply feeling to the lower half of the body.
The medication is injected into a sac of fluid in your lower back (the subarachnoid space) which contains the spinal nerves.
The medication blocks the nerves in the lower half of the body. The loss of feeling is temporary and should last from 1 to 4 hours depending on the medication given and other factors
وهي عن طريق حقن ابرة رفيعة جدا وجرعة واحدة في السائل او ال
SUBARACHNOID SPACE اي في السائل المحيط بالحبل الشوكي وهي تحتاج الى نسبة بسيطة جدا من جرعة التخدير لانها تؤدي الى التخدير الجزء السفلي من الجسم
epidural anesthesia, a form of regional anesthesia involving injection of drugs through a catheter placed into the epidural space. The injection can cause both a loss of sensation (anaesthesia) and a loss of pain (analgesia), by blocking the transmission of signals through nerves in or near the spinal cord.
Difference from spinal anesthesia
-The involved space is larger for an epidural, and subsequently the injected dose is larger, being about 10-20 ml in epidural anesthesia compared to 1,5-3,5 ml in a spinal.
-In an epidural, an indwelling catheter may be placed that avails for additional injections later, while a spinal is a one-shot only.
-The onset of analgesia is approximately 15-30 minutes in an epidural, while it is approximately 5 minutes in a spinal.
-An epidural usually doesn't cause significant neuromuscular block, while a spinal more often does. An epidural may be given at a thoracic or lumbar site, while a spinal must be injected below L2 to avoid piercing the spinal cord.
صورة توضح مكان دخول الابرة بين فقرات الظهر في الغضروف بعيدا عن الاعصاب
1- الحقن في وضع الجلوس :
يجلس المريض على منضدة العمليات مريحا قدميه على مقعد صغير مع ثني العمود الفقري بحيث يأخذ الظهر سطحا محدبا وذلك بضغط الذقن على عظمة القص
. فبذلك تبرز الزوائد أو النتوءات الشوكية ( Spinous Processes ) بوضوح كما تتسع المسافة بين الفقرات ويساعد على الوصول إلى هذا الوضع لو ضغطنا أيضا على البطن عند الصرة .
ثم يعقم ويطهر موضع الحقن بصبغة اليود أو الميكركروم الكحولي
- وبعد تجفيف المكان الذي ستؤخز فيه الإبرة الخاصة بالتخدير النصفي ( Spinal Needle ) فتخرق الجلد والأغشية تحت الجلدية ثم الأربطة التي توصل بين نتوءات الفقرات حتى تصل إلى المسافة خارج الام الجافية – ثم الام الجافية والعنكبوتية لتصل إلى المسافة تحت العنكبوتية والتي يجري فيها السائل النخاعي حيث يتم الحقن بالسائل المخدر.
Position of the patient
The patient may be in the sitting position or lateral position (lying on one side). The sitting patient is asked to slouch and bend forward slightly from the waist to increase the curvature of the spine. The lying patient is asked to draw the knees up to the chin for the same reason.
طريقة إعطاء التخدير النصفي
ب- الحقن في الوضع الجانبي :
ينام المريض على جانبه فوق منضدة العمليات بحيث يكون ظهره على حافة المنضدة وتنثني الركبتين على البطن – والرأس إلى الركبتين – مع ملاحظة أن مفاصل الحوض والكتف تكون عمودية على المنضدة - ونختار هذا الوضع إذا أردنا التخدير على جانب واحد من الجسم – وعندئذ يكون جانب المريض هو الملتصق بمنضدة العمليات عند استعمال السوائل المخدرة الثقيلة والجانب السليم هو الملتصق بالمنضدة عند استعمال السوائل المخدرة ذات الثقل النوعي الخفيف
Anaesthetic drugs
A patient receiving an epidural for pain relief typically receives a combination of local anesthetics and opioids. This combination works better than either type of drug used alone. Common local anesthetics include lidocaine, bupivacaine, ropivacaine, and chloroprocaine. Common opioids include morphine, fentanyl, sufentanil, and pethidine . These are injected in relatively small doses
.
Contraindications
Absolute
Patient refusal
Coagulopathy.
Insertion of an epidural needle or catheter into the epidural space may cause traumatic bleeding into the epidural space. Clotting abnormalities may lead to the development of a large haematoma leading to spinal cord compression.
Therapeutic anticoagulation.
( see later)
Skin infection at injection site.
Insertion of the epidural needle through an area of skin infection may introduce pathogenic bacteria into the epidural space, leading to serious complications such as meningitis or epidural abscess.
Raised intracranial pressure.
Accidental dural puncture in a patient with raised ICP may lead to brainstem herniation (coning).
Hypovolaemia.
The sympathetic blockade produced by epidurals, in combination with uncorrected hypovolaemia, may cause profound circulatory collapse.
Relative
Uncooperative patients
may be impossible to position correctly, and be unable to remain still enough to safely insert an epidural.
Pre-existing neurological disorders,
such as multiple sclerosis, may be a contraindication, because any new neurological symptoms may be ascribed to the epidural.
Fixed cardiac output states.
Probably relative rather than absolute. This includes aortic stenosis, hypertrophic obstructive cardiomyopathy (HOCM), mitral stenosis and complete heart block. Patients with these cardiovascular abnormalities are unable to increase their cardiac output in response to the peripheral vasodilatation caused by epidural blockade, and may develop profound circulatory collapse which is very difficult to treat.
Anatomical abnormalities of vertebral column may make the placement of an epidural technically impossible.
Prophylactic low dose heparin
Regional anesthesia and anticoagulants
Full oral anticoagulation with warfarin or standard heparin (SH) are absolute contraindications to epidural blockade.
Partial anticoagulation with low molecular weight heparin (LMWH) or low dose warfarin (INR <1.5) are relative contraindications.
Low dose standard heparin (SH), 5,000units bd s/c is not associated with an increased risk of epidural haematoma. Wait for 4 hours after a dose before performing epidural.
LMWH : allow 12hr interval between LMWH administration and epidural; this also applies to removal of epidural catheters.
NSAID's (including aspirin) do not increase the risk of epidural haematoma.
Intraoperative anticoagulation using 5000units i/v heparin following epidural/spinal injection appears safe, but careful postoperative observations are recommended. .
Fibrinolytic and thrombolytic drugs: avoid epidural block for 24 hrs, check clotting prior to insertion.
Thrombocytopaenia: epidurals are relatively contraindicated below platelet count of 100,000/mm3.
An epidural haematoma should be suspected in patients who complain of severe back pain a few hours/days following any central neuraxial block or with any prolonged or abnormal neurological deficit (including. sensory loss, paraesthesiae, muscle weakness and disturbance of bladder control and anal sphincter tone). A high index of suspicion is required, with early orthopaedic or neurosurgical referral for decompression of the haematoma. Even with early recognition, the morbidity of this condition is still very high
Important complications of regional anaesthesia
Pain - 25% of patients still experience pain despite spinal anaesthesia
Post-dural headache from CSF leak
Hypotension and bradycardia through blockade of the sympathetic nervous system
Limb damage from sensory and motor block
Epidural or intrathecal bleed
Respiratory failure if block is 'too high'
Direct nerve damage
Hypothermia
Damage to the spinal cord - may be transient or permanent
Spinal infection
Aseptic meningitis
Haematoma of the spinal cord - enhanced by use of LMWH preoperatively
Anaphylaxis
Urinary retention
و يتميز التخدير النصفي بما يلي
:
يجنب المريض بعض الآثار السيئة للمواد المستخدمة فى التخدير الكلي و لا سيما فى مرضى القلب و الكبد و الجهاز التنفسي
.
يساعد على تقليل ضغط الدم مما يساعد على تقليل النزف فى جراحات الفخذ (لا يوجد نزف فى جراحات الركبة لأنه يتم وضع رباط على الفخذ يمنع وصول الدم للركبة أثناء الجراحة
).
لا يحتاج المريض لوقت للإفاقة من التخدير و يستطيع الأكل و الشرب بعد إجراء الجراحة مباشرة و لا يوجد ميل للقيء
.
تساعد على تقليل الألم بعد الجراحة حيث يمكن تركيب أنبوب رفيع للغاية يتم من خلاله حقن المواد المخدرة بعد الجراحة



» ultrasound of lung in critical care patients
» respiratory diseases , anaesthetic management 2023
» thoracic anaesthesia 2023
» indication to SICU admission
» electrolyte disturbances
» fluid physiology
» TAP block USG
» Assisted ventilation for surgical patients
» nutrition in critical ill patient
» US workshop in Mosul
» Basics of ultrasound
» الملتقى العلمي الاول للجمعية العراقية للتخدير والعناية المركزة والحد من الالم فرع الموصل
» Geriatric anaesthesia
» thoracic anaesthesia 2022
» chronic pain management
» anaesthesia in respiratory diseases
» anaesthesia for plastic procedures
» ECG for candidate
» postoperative care